

Q: I broke my collarbone riding my dirt bike. The local hospital put me in a sling and sent me on my way, but now an orthopedic specialist says I need to get it plated. What are my options?
OK, you crashed. Maybe it was during your first off-road jaunt, or taking off with a new cold rear tire around a slick corner. First, you’re alive — that’s great — but don't feel too special about your fracture. A broken collarbone (fractured clavicle) is extremely common for riders of two-wheeled vehicles, including bicycles and motorcycles, regardless of on- or off-road setting. Second, for the most part, these kinds of injuries heal phenomenally well. Third, when your fracture is properly healed, you can go back to riding again!
In the realm of potential injuries after a crash, this one is not so bad. You could even do without a collarbone entirely (yup, sometimes we take it out — but that would be exceedingly rare to manage a fracture)! Let's look at your collarbone.
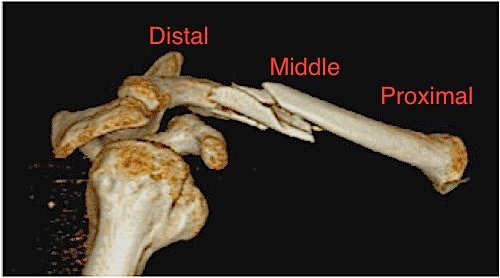
Major issues with these fractures include, in order of occurrence, pain, deformity, limited range of motion or strength, non- or mal-union (lack of healing of bony ends or poor/incomplete healing — most common in distal fractures), injury to underlying structures (blood vessels, covering of lung, lung). If the fracture fragments protrude through the skin, it is called an open fracture and has an increased risk of infection. Since the collarbone provides linkage between your sternum and your shoulder, it functions a lot like a car’s strut assembly. When your collarbone is broken, it can reduce your strength and range of motion around your shoulder joint, since it weakens that linkage.
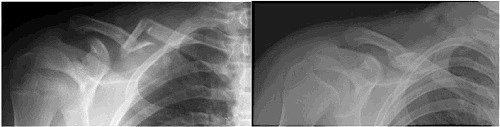
We now know that we can be similarly effective placing the arm on the side of the fracture in a sling, instead. This is the most common method of management for middle third fractures that are reasonably well aligned. When the ends heal together, they do so by laying down additional calcium in a supportive framework that you can feel with your fingers as a lump and see on an x-ray as a bonelike mass called a callus. Yes, it is just about as strong as your bone before the break. The average time between fracture and healing to allow you to safely resume riding is six weeks. If you are thin, you may be able to see that the healed side looks a little different from the uninjured one. Since most of us are not runway models, the cosmetic abnormality is a curiosity, but not something to fix.

The current question, however, is whether the success of operative management should also be applied to all or some of the fractures that could heal perfectly well on their own. Unlike the robust data that helps us understand who should take an aspirin a day, or whether or not ongoing rider training has utility, there is not a lot of data to help decide about plating your clavicle fracture. The technique has been around for more than 20 years, but trials comparing operation versus sling have few patients and are generally limited to middle third fractures. A recent trial (ages: 5 to 21) examined less than 100 patients in total and concluded that both approaches were equivalent. Similar findings have been noted in adults in several comparisons. While new drug trials need only prove that the new drug isn’t worse than the one already in use, trials of operative techniques should demonstrate a benefit, since the operation generally includes additional risks you don't have without operation. Complications have been well described after operation, many of which, in retrospect, are believed to be avoidable.
So what should you do? Since there is not a single best approach for the overwhelming majority of these fractures, an individualized approach is appropriate. This means that you need to discuss with your doctor the options, risks, benefits and potential complications of both approaches and together decide what is best for you.
Remember that every operation also “buys” you the risks of anesthesia, infection at the site of operation, injury to surrounding structures, and the potential for another operation, especially in the event of infection. Hardware (the metal plates and the screws, and sometimes wires) can also become infected, loosen, and may need to be removed. Operations like a plate and screws may be simple for your surgeon, but carry important and measurable risk that should be balanced against the benefits of the procedure. This is an important part of your discussion and is similar to evaluating the benefits of the upgraded options for your new bike against the downsides of the sucking sound made by money leaving your wallet.
Now you have more information to help you make an informed decision — the goal of talking to your doctor!
Image Gallery








